Overview
During contraction of the calf muscle, tension is placed through the Achilles tendon and this rubs against the retrocalcaneal bursa. Compressive forces and friction may also be placed on the retrocalcaneal bursa during certain ankle movements or by wearing excessively tight shoes. When these forces are excessive due to too much repetition or high force, irritation and inflammation of the bursa may occur. This condition is known as retrocalcaneal bursitis.
Causes
For the most part, it is a genetic condition. You develop it by inheriting a foot type that is prone to the mechanical irritation that leads to the problem. If you have this particular foot type and wear shoes that rub and irritate the back of the heel bone (calcaneus) where the Achilles tendon attaches, then you are even more likely to develop this type of bursitis. The contributing factors include a supinated foot type, a heel bone with a prominence (or pointed shape that stick out toward the tendon) at the back, a tight Achilles tendon (referred to as Equinus by doctors), and a high arch. All of these factors simply make it more likely that the back of the heel will press against the shoe and rub. As the tendon gets rubbed the wrong way, the bursa starts to develop and fill with fluid. This response is really your body’s way of protecting the tendon from damage, but it backfires. The friction from all that rubbing causes the bursa to become inflamed and swell. This causes the bump to become red, hot and stick out even further. Much like a sore thumb, it then gets irritated by even the softest shoes.
Symptoms
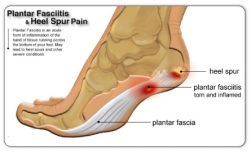
Below is a list of common signs and symptoms of retrocalcaneal bursitis. Recognizing and treating symptoms early can prevent retrocalcaneal bursitis from becoming chronic. Swelling. The retrocalcaneal bursa is located behind the Achilles tendon, just above where the tendon attaches to the heel bone. When the bursa is inflamed it will cause visible soft tissue swelling near the top of the heel bone. It is worth noting that bursitis of the retroachilles bursa, which is located between the Achilles tendon and skin, can manifest slightly differently: swelling may be more distinct, appearing as a hard lump behind the heel. Retroachilles bursitis is also more likely than retrocalcaneal bursitis to cause the skin at the back of the heel to turn red.
Diagnosis
Before making a diagnosis of retrocalcaneal bursitis, a doctor must rule out other possible problems, such as arthritis, a fracture or tumor. A doctor also will try to determine if the Achilles tendon itself is a source of pain. To make a diagnosis, a doctor will use some or all of the diagnostic tools below Patient interview. A doctor will ask a patient about medical history, and to describe the onset of his or her symptoms, the pattern of pain and swelling, and how symptoms affect lifestyle. For example, doctors may ask patients what types of shoes they wear and what they do for exercise. A patient’s reported symptoms are important to diagnosis and treatment. The doctor will also ask what home treatments have helped the condition. Physical exam. A doctor will examine the patient’s foot, noting swelling, tenderness and pain points, and range of motion. The doctor also may ask the patient to point and flex the feet and stand on his or her toes.
Non Surgical Treatment
If you follow these steps, most attacks of bursitis should subside in four or five days and all symptoms should be gone within two weeks. Rest the body part that hurts. If you suspect that one activity has caused the pain, stop it until the pain is entirely gone. A sling, splint, or padding may be needed to protect the area from possible bumps or irritation. Try over-the-counter pain relievers. Nonprescription NSAIDs (aspirin, ibuprofen, and naproxen) will help reduce pain and swelling, though they won?t accelerate healing. Acetaminophen will help with pain but it doesn?t reduce inflammation. Ice it, then heat it. Apply ice packs during the first two days to bring down swelling. Then use heat-warm baths or a heating pad (on a medium or low setting)-to ease pain and stimulate blood flow. Don?t push it. Resume exercising only after you feel better. Start with gentle activity. Skip the liniments. Liniments and balms are no help for bursitis. Liniments don?t penetrate deeply enough to treat bursitis, they mainly warm the skin and make it tingle, thus distracting attention from the pain beneath. Massage is likely to make matters worse. Undergo physical therapy. Physical therapy strengthens joint muscles that have been affected by bursitis and may help prevent the bursitis from getting worse.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
 Overview
Overview Symptoms
Symptoms Prevention
Prevention Overview
Overview Symptoms
Symptoms


 Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It’s also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor’s supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It’s also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor’s supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.






